What is Peyronie's disease?
It most commonly occurs in middle aged men but can occur in both younger and older men. It occurs in up to 3-9% of men but most people have never heard of it.
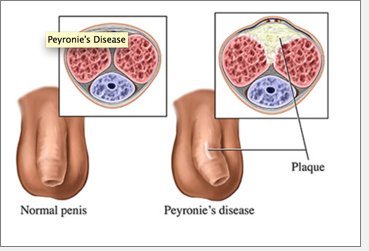
Peyronie’s disease is caused by scarring of the tunica albuginea or thrmembrane that surrounds the muscle of the penis. It is characterised by a penile bend, lump and pain on erection. There are two phases of the disease; an acute phase lasting about 3-6 months followed by a chronic phase lasting up to about a year during which the disease usually stabilises.It is believed that most cases of Peyronie’s disease result from either sexual and / or repetitive trauma to the penis but may equally may be linked to vascular disease. However, the exact cause of the disease remains unknown.
Symptoms
Usually the plaque forms on the top of the shaft, making the penis bend upward. But if the plaque is on the underside it will bend downward. In some cases, the plaque develops on both top and bottom, leading to indentation and shortening of the penis.
In the worst cases, the hardened plaque reduces flexibility and causes so much pain, bending and emotional distress that sex becomes impossible.
Causes and risk factors
The cause of Peyronie's disease isn't fully understood. There's a link to fibrosis or scarring of other tissues in the body such as a condition known as Dupuytren's contracture of the hand. There's also a mild family tendency to the disease. It is also found to be associated with Diabetes in 30% of cases.
Many researchers believe the plaque or lump in Peyronie's disease develops following repeated trauma such as hitting or bending that causes localised bleeding inside the penis. This leads to injury of the elastic lining of chambers inside the penis.
Ageing increases the risk as a general reduction in elasticity of the body's tissues increases the chances of injury. If the damaged area heals slowly, the plaque undergoes fibrosis, or formation of tough fibrous tissue, and even calcification (formation of calcium deposits) resulting in a long-term problem.
But this theory doesn't explain those cases which develop slowly, or why similar conditions such as Dupuytren's contracture don't seem to result from severe trauma.
Peyronie's disease often occurs in a mild form that stops progressing without treatment after six to 18 months. However, for some men the problem is severe and disabling with regards to erections.
The main aim of treatment is to help the man stay sexually active. We try to avoid medical treatment as there is no strong evidence to show that any treatment other than surgery is effective. For many patients information and reassurance from an expert may be all that is required.
Surgery is usually performed after 12 months when the disease is stabilised and the deformity prevents intercourse. Because the symptoms of Peyronie's disease can improve without treatment, it is important to wait at least 6-12 months to allow the disease to stabilise before attempting to correct it surgically.
Does Peyronie's Disease Require Surgery?
In most cases Peyronie’s disease does not require any surgery. The only indication for surgical treatment is the inability to penetrate and have intercourse, or difficulty with intercourse. Usually this occurs if a bend is 30-45 degrees or greater, although it can occur with lesser bends such as those where it bends to the side.
Other currently unproven treatments available include:
• Vitamin E tablets.
• Para-aminobenzoate tablets.
• Injections of chemical agents such as collagenase, steroids and calcium channel blockers directly into the plaques (the most promising being collagenase, an enzyme that attacks collagen, the major component of Peyronie's plaques).
• Shockwave lithotripsy therapy has also been used but, while it can reduce pain, the results have been very variable.
• More recently, a novel drug called Xiaflex, which is a collagenase has undergone trials and appears to be promising for the treatment of Peyronie’s disease, although is currently available in the UK.
• In those men who do not respond to medical treatment , surgery can be offered if the bend prevents sex.
Surgical Techniques for Peyronie's Disease
Many surgical techniques have been advocated for the treatment of Peyronie’s Disease. Some of these involve shortening the penis on the opposite side to the bend, the so called Nesbit’s procedure, or plication procedures. Grafting of the scarred area is also possible but it is important to note that the plaque is usually incised and a graft placed over the area. All of these types of surgery can result in complications.
The following surgical operations for Peyronie’s disease:
• If there is a deformity of greater than 45 degrees; incision or expansion of the plaque followed by placement of a patch of vein or collagen matrix (‘Lue’ procedure). This has a higher rate of maintaining the length of the penis. However, it can involve partial loss of erectile function, especially rigidity, and has a higher rate of complications than the Nesbit operation (see below).
• If the deformity is less than 45 degrees; removal or pinching of tissue from the side of the penis opposite the plaque, which cancels out the bending effect (‘Nesbit’ procedure). This invariably causes a shortening of the erect penis. After operative intervention, the deformity can sometimes recur and then a Lue procedure may need to be performed.
• If there is significant erectile dysfunction (that cannot be improved with medical therapy) associated with penile deformity, implantation of a penile implant device that increases rigidity of the penis. In some cases, an implant alone will straighten the penis adequately. In other cases, implantation is combined with a technique of incisions and grafting or plication (pinching or folding the skin).
What happens during Surgery?
When patients have surgery for Peyronie’s Disease the penis is degloved through a circumferential incision around the head of the penis. An artificial erection is induced with saline. At the time of surgery, a catheter is inserted into the urethra to ensure that patients are able to void after surgery and furthermore there is no damage to the urethra (‘water-pipe’) during such surgery. The catheter is usually removed the following day unless the urethra is mobilised to correct the bend.
Patients are then asked to abstain from sexual intercourse for approximately six weeks after surgery so that the reconstruction has time to heal. After surgery patients commence drugs such as Cialis or Viagra to try and stimulate and stretch the penis post operatively. In some cases a vacuum erection device may be used to stretch the penis to try and reduce the risk of penile shortening.
Complications of Surgery
The most common complications following surgery are shortening to the penis, erectile dysfunction and changes in sensitivity to the penis. In some cases patients may require a circumcision particularly if their foreskin is very tight.
In some cases, patients who have pre-existing erectile dysfunction and have had medical treatments to correct this may require a penile implant to treat Peyronie’s disease. Penile implants or prosthesis are the treatment of choice because they straighten the penis and correct erectile dysfunction. Patients require extensive counselling before such surgery.
|




